MKSAP Quiz: Worsening chronic shoulder pain
An 85-year-old woman is evaluated for worsening chronic right shoulder pain of 1 year's duration. The pain is more severe with use. She has no history of trauma to the shoulder.
On physical examination, vital signs are normal. The right shoulder is swollen and tender, with no warmth or redness. There is pain-related decreased range of motion of the shoulder in all directions. Other joints are normal.

Erythrocyte sedimentation rate and blood C-reactive protein level are normal.
Radiograph of right shoulder is shown.
Synovial fluid from the right shoulder is blood-tinged; analysis of fluid reveals a leukocyte count of 500/μL (0.5 × 109/L), negative Gram stain and culture results, and no crystals.
Which of the following is the most likely diagnosis?
A. Adhesive capsulitis
B. Basic calcium phosphate–associated arthritis
C. Calcium pyrophosphate deposition disease
D. Rheumatoid arthritis
Answer and critique
This content is available to MKSAP subscribers as Question 35 in the Rheumatology section.
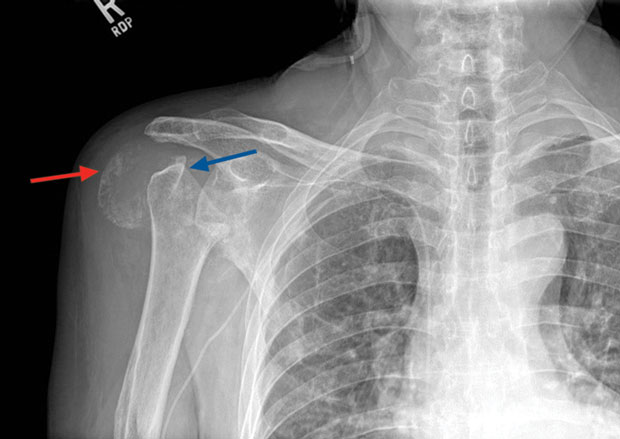
The most likely diagnosis is basic calcium phosphate–associated arthritis (Option B). Deposition of basic calcium phosphate crystals (hydroxyappatite) occurs in older persons and targets periarticular tendons and ligaments. In rare instances, basic calcium phosphate crystal deposition is associated with inflammatory arthritis and periarthritis, most classically manifesting in older women as "Milwaukee shoulder." This inflammatory state causes progressive destruction of the glenohumeral joint, and destruction of the rotator cuff as shown in the radiograph. The blue arrow, pointing to the humeral head, illustrates aggressive bone destruction at the glenohumeral junction. The red arrow illustrates distended subacromial/subdeltoid bursa with fluid and calcific debris. Basic calcium phosphate crystals are not seen on routine synovial fluid analysis because visualization requires special stains and/or electron microscopy. Unlike in other crystal-induced diseases, pain onset is gradual.
Adhesive capsulitis (frozen shoulder) (Option A) usually occurs in patients aged 40 to 70 years. The cause appears to involve glenohumeral joint capsular thickening and fibrosis. Patients describe shoulder pain that is often constant but is worse at night and in cold weather; shoulder stiffness is common. Adhesive capsulitis can be idiopathic but is also associated with prolonged immobilization, antecedent shoulder surgery or injury, diabetes mellitus, hypothyroidism, and autoimmune disorders. On examination, patients have limited passive and active range of motion in all directions. Plain radiographs are of limited diagnostic use in patients with adhesive capsulitis; most often the radiographs are normal, except for osteopenia in some cases. This patient's abnormal shoulder radiograph is not consistent with adhesive capsulitis.
Calcium pyrophosphate deposition (CPPD) disease (Option C) is an unlikely diagnosis. Although it may involve the shoulder joint, it is typically associated with osteoarthritis, not severe erosive joint destruction. Calcium pyrophosphate crystals, which are weakly positively birefringent (blue when parallel to and yellow when perpendicular to the polarizing axis of an optical filter) and classically rhomboid-shaped, are usually identified in the joint fluid. Chondrocalcinosis, visible as a thin white line that tracks below the surface layer of the cartilage within the joint, may be visible on plain radiograph. Extensive soft-tissue calcification such as seen in this radiograph is not typical of CPPD.
Rheumatoid arthritis (Option D) rarely presents in the shoulder in older patients. It is associated with inflammatory joint fluid (leukocyte count, 2000-20,000/μL [2.0-20 × 109/L]) and is not associated with periarticular calcifications on plain radiographs. Monoarticular presentations of rheumatoid arthritis are uncommon.
Key Points
- Deposition of basic calcium phosphate crystals (hydroxyappatite) occurs in older persons and targets periarticular tendons and ligaments.
- In rare instances, basic calcium phosphate crystal deposition is associated with inflammatory arthritis and periarthritis, most classically manifesting in older women as "Milwaukee shoulder," an inflammatory state that causes progressive destruction of the rotator cuff and glenohumeral joint.

