MKSAP Quiz: Hospitalization for increasing shortness of breath
A 24-year-old woman is hospitalized for increasing shortness of breath, fatigue, productive cough, and pleuritic chest pain of 2 weeks' duration; she has also been experiencing fever and chills for the past month. She has rheumatoid arthritis diagnosed 4 years ago. She lives in northern Georgia. Her medications are methotrexate, etanercept, low-dose prednisone, and ibuprofen as needed.
On physical examination, temperature is 39.2 °C (102.6 °F), blood pressure is 125/60 mm Hg, pulse rate is 128/min, and respiration rate is 26/min. Bilateral crackles are heard in the lungs. Abdominal examination reveals hepatosplenomegaly. Minimal synovitis is present in the wrists and metacarpophalangeal joints bilaterally.
Laboratory studies show a hemoglobin level of 7.5 g/dL (75 g/L), leukocyte count of 4500/µL (4.5 × 109/L), and platelet count of 50,000/µL (50 × 109/L).
Chest radiograph shows bilateral reticulonodular infiltrates.
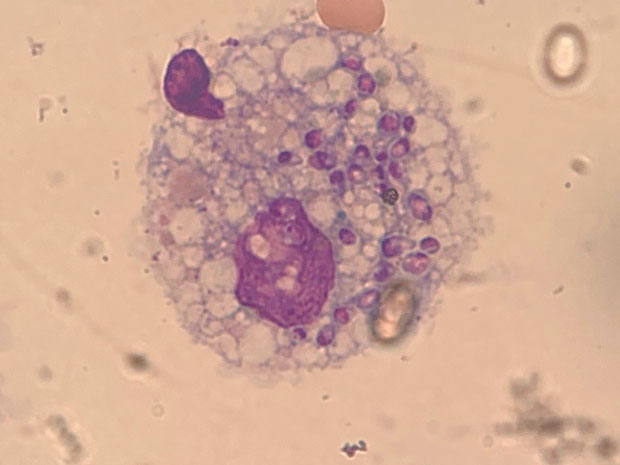
Blood cultures are negative. Peripheral blood smear is shown.
The Histoplasma urinary antigen assay is positive.
Which of the following is the most appropriate treatment?
A. Fluconazole
B. Itraconazole
C. Liposomal amphotericin B
D. Posaconazole
Answer and critique
This content is available to MKSAP 19 subscribers as Question 33 in the Infectious Disease section.
The most appropriate treatment for this patient is liposomal amphotericin B (Option C) for disseminated histoplasmosis. The Histoplasma urinary antigen assay has a sensitivity and specificity of greater than 85% in acute and disseminated infection but less than 50% in chronic infection. Identification of the fungus by tissue culture can be a lengthy process but is indicated for clinically suspected cases in which the urinary antigen assay result is negative. The peripheral blood smear also shows yeast cells within a leukocyte, characteristic of disseminated histoplasmosis. Furthermore, the patient has several risk factors, including living in an endemic area and taking immunosuppressant medication; treatment with tumor necrosis factor-α inhibitors (e.g., infliximab, etanercept, adalimumab) is an increasingly recognized cause of disseminated histoplasmosis in patients with rheumatoid arthritis. The abnormal chest radiograph with bilateral infiltrates and hepatosplenomegaly also indicate infection with Histoplasma. Finally, thrombocytopenia and anemia are also characteristic of histoplasmosis. If disseminated histoplasmosis is not diagnosed and treated early, patients can develop septic shock, which has a mortality rate as high as 90%. The treatment of choice remains liposomal amphotericin B; however, oral itraconazole can be used to complete therapy after improvement is shown.
Fluconazole (Option A) has been used in patients with histoplasmosis who could not take amphotericin B or itraconazole. However, fluconazole is not as effective as either amphotericin B or itraconazole and clears fungemia more slowly. The development of resistance also makes fluconazole a much less desirable therapy.
Itraconazole (Option B) can be used as monotherapy for patients with mild to moderate disease caused by histoplasmosis. However, itraconazole does not clear fungemia as quickly as amphotericin B and is, therefore, not a first-line agent in patients with severe or disseminated histoplasmosis.
Posaconazole (Option D) is a triazole antifungal used to treat many invasive fungal infections, including aspergillosis and mucormycosis. However, it has not been fully evaluated in any form of histoplasmosis. It may be useful in certain situations when itraconazole or liposomal amphotericin B cannot be used, but it is not a first-line treatment choice.
Key Points
- The Histoplasma urinary antigen assay has a sensitivity and specificity of greater than 85% in acute and disseminated infection.
- The treatment of choice for disseminated histoplasmosis is liposomal amphotericin B.


