MKSAP Quiz: 1-week history of sore throat, odynophagia
A 30-year-old man is evaluated for a 1-week history of sore throat and odynophagia. He reports no fever, nausea, vomiting, diarrhea, or other symptoms. He was recently diagnosed with HIV infection and began antiretroviral therapy 2 weeks ago. Medications are tenofovir alafenamide, emtricitabine, dolutegravir, and trimethoprim-sulfamethoxazole.
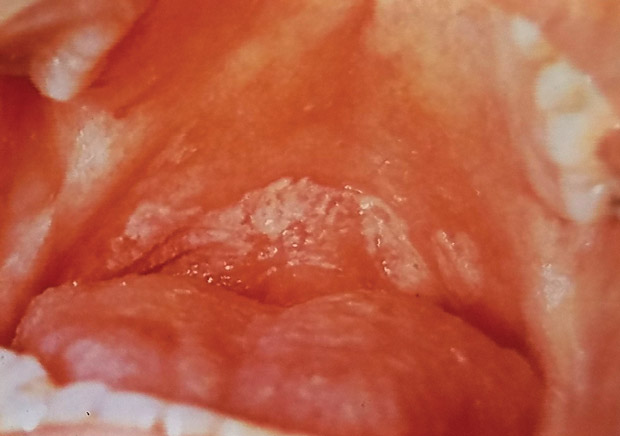
On physical examination, vital signs are normal. Oral examination findings (shown) include whitish plaques on the posterior pharynx. Lymph nodes are palpable in the anterior and posterior cervical regions bilaterally. The remainder of the examination is normal.
Laboratory studies at the time of HIV diagnosis showed a CD4 cell count of 55/µL and HIV viral load of 138,855 copies/mL.
Which of the following is the most appropriate management?
A. Intravenous caspofungin
B. Oral fluconazole
C. Nystatin swish-and-swallow
D. Upper endoscopy
E. Valganciclovir
Answer and critique
The correct answer is B. Oral fluconazole. This item is Question 96 in MKSAP 18's Infectious Disease section.
Oral fluconazole is the most appropriate management for this patient's likely esophageal candidiasis; he should be treated presumptively and followed for response. The diagnosis of oropharyngeal candidiasis is usually made clinically; although whitish plaques are often prominent, oral candidiasis may also present as diffuse erythema without plaques. The presence of oral candidiasis and painful swallowing symptoms indicates likely esophageal involvement. The preferred treatment is oral fluconazole regardless if the disease is isolated to the oral cavity or extends into the esophagus; however, esophageal involvement warrants a more prolonged course (14-21 days rather than 7-14 days). Clinical response is usually apparent within a few days.
Because this patient is able to swallow pills, oral therapy is appropriate, and intravenous therapy is unnecessary. Additionally, fluconazole has higher rates for complete resolution without relapse of disease than the echinocandins and is preferred therapy unless resistance is documented, which would not be expected in a patient who has not been taking long-term azole therapy.
Topical agents such as nystatin are less effective than systemic fluconazole for oropharyngeal candidiasis and are especially ineffective for esophageal disease.
If presumptive treatment for candida esophagitis is ineffective in improving symptoms, then upper endoscopy is indicated to better define the cause.
Cytomegalovirus esophagitis is seen in immunocompromised patients and rarely occurs in patients with an intact immune system. Although herpes simplex virus (HSV) esophagitis can be seen in immunocompetent and immunocompromised patients, it is much more likely to be found in an immunocompromised person. These viral infections usually manifest as esophageal ulcerative lesions rather than plaques. Biopsies of the ulcer should be performed to confirm cytomegalovirus and HSV. Treatment of cytomegalovirus with valganciclovir (or HSV with acyclovir) would not be appropriate without first seeing evidence for it on endoscopy.
Key Point
- The preferred treatment for oropharyngeal candidiasis, including esophageal disease, is oral fluconazole, although esophageal involvement warrants a more prolonged treatment course.



