MKSAP Quiz: Episode of blood in urine
A 37-year-old woman is evaluated for an episode of blood in her urine. She notes the passage of red-colored urine that resolved spontaneously and was not associated with her menstrual cycle. She reports having had several similar episodes in the past. She has no other symptoms such as abdominal pain or dysuria. Medical history is otherwise unremarkable, and she takes no medications.
On physical examination, the patient is afebrile. Blood pressure is 128/78 mm Hg, pulse rate is 82/min, and respiration rate is 13/min. Cardiopulmonary and abdominal examinations are normal. There is no flank tenderness to palpation. The remainder of the examination is unremarkable.
Laboratory studies show a normal complete blood count and metabolic profile and a serum creatinine level of 0.9 mg/dL (79.6 µmol/L). Dipstick urinalysis is positive for blood and protein but is negative for leukocyte esterase and nitrites.
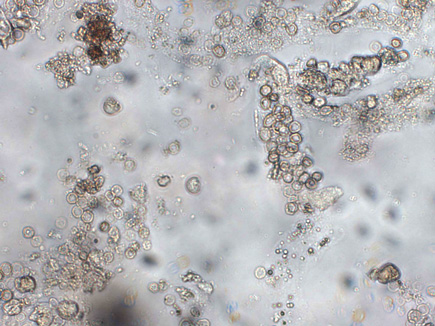
Microscopy of the urine sediment is shown.
Which of the following is the most appropriate next step in the evaluation of this patient?
A. Cystoscopy
B. Evaluation for glomerular disease
C. Noncontrast helical abdominal CT
D. Serum creatine kinase measurement
Answer and critique
The correct answer is B. Evaluation for glomerular disease. This question can be found in MKSAP 17 in the Nephrology section, item 8.
Evaluation for glomerular disease is the most appropriate next step for this patient. An initial step in evaluating hematuria is assessing whether the likely source of bleeding is from the glomerulus or elsewhere in the urinary tract. Glomerular hematuria is typically characterized by brown- or tea-colored urine with dysmorphic erythrocytes (or acanthocytes) and/or erythrocyte casts on urine sediment examination, although some glomerular disorders may cause gross hematuria. Other findings suggestive of a glomerular source include proteinuria. Nonglomerular bleeding typically presents with isomorphic erythrocytes in the urine without evidence of glomerular dysfunction. Glomerular causes of hematuria include inflammatory processes such as glomerulonephritis that may lead to rapid declines in kidney function but may also include more benign or indolent diseases such as thin glomerular basement membrane disease, IgA nephropathy, and other forms of chronic glomerulonephritis. The clinical presentation in this asymptomatic patient with normal kidney function and apparent recurrent episodes of gross hematuria is consistent with IgA nephropathy as a cause of her hematuria.
Cystoscopy is used to evaluate for lower urinary tract causes of nonglomerular bleeding. It is not an appropriate next step in this patient with evidence of glomerular bleeding and no other risk factors for lower urinary tract pathology.
Noncontrast helical abdominal CT can be used to detect kidney stones or other potential causes of nonglomerular hematuria. However, this patient's presentation is not suggestive of nephrolithiasis, and she has evidence of a glomerular source of her hematuria. Additionally, the preferred method of kidney imaging in younger patients, particularly women of childbearing age, is ultrasonography due to decreased radiation exposure.
Measurement of serum creatine kinase levels is useful in evaluating for rhabdomyolysis. This diagnosis should be suspected when dipstick urinalysis is positive for heme with a negative microscopic urinalysis for erythrocytes; however, this patient has evidence of erythrocytes in her urine. Additionally, she does not have a clinical history consistent with rhabdomyolysis, and her urine studies suggest a glomerular cause of her hematuria.
Key Point
- Glomerular hematuria typically features brown- or tea-colored urine with dysmorphic erythrocytes (or acanthocytes) and/or erythrocyte casts on urine sediment examination.



