MKSAP Quiz: Evaluation for palpitations
A 28-year-old woman is evaluated after a 4-hour self-limited episode of palpitations. The symptoms occurred while at work yesterday. She has no history of cardiovascular disease and has no other cardiovascular symptoms. She is active without limitations. She is on no medications.
On physical examination, blood pressure is 110/70 mm Hg, pulse rate is 60/min and regular, and respiration rate is 15/min. BMI is 23. The estimated central venous pressure is elevated. The apical impulse is normal; there is a parasternal impulse present at the left sternal border, and a soft midsystolic murmur is heard at the second left intercostal space. Fixed splitting of the S2 is noted throughout the cardiac cycle. The remainder of the physical examination is normal.
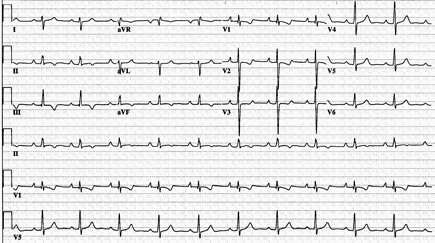
Electrocardiogram is shown.
Which of the following is the most likely diagnosis?
A. Atrial septal defect
B. Bicuspid aortic valve with aortic stenosis
C. Congenital pulmonary valve stenosis
D. Mitral valve prolapse with mitral regurgitation
Answer and critique
The correct answer is A: Atrial septal defect. This question can be found in MKSAP 17 in the Cardiovascular Medicine section, item 29.
This patient has features of an ostium secundum atrial septal defect. Adults with atrial septal defects often present with atrial arrhythmias. The characteristic physical examination findings in atrial septal defect are fixed splitting of the S2 and a right ventricular heave. A pulmonary midsystolic flow murmur and a tricuspid diastolic flow rumble caused by increased flow through the right-sided valves from a large left-to-right shunt may be heard. In ostium secundum atrial septal defect, the electrocardiogram (ECG) demonstrates right axis deviation and incomplete right bundle branch block. Ostium primum atrial septal defects are nearly always associated with anomalies of the atrioventricular valves, particularly a cleft in the anterior mitral valve leaflet or defects of the ventricular septum. The ECG in ostium primum atrial septal defect characteristically demonstrates first-degree atrioventricular block, left axis deviation, and right bundle branch block.
Bicuspid aortic valve with aortic stenosis causes a systolic murmur at the second right intercostal space. The central venous pressure is normal in aortic stenosis, and a right ventricular impulse would not be expected. Fixed splitting of the S2 is not heard in patients with bicuspid aortic valve with aortic stenosis. The ECG typically demonstrates a normal axis and features of left ventricular hypertrophy.
Patients with pulmonary valve stenosis may demonstrate jugular venous pressure elevation with prominence of the a wave and a parasternal impulse from increased right ventricular pressure. The ejection murmur of pulmonary valve stenosis is heard at the second left intercostal space, and the timing of the peak of the murmur is related to stenosis severity. An ejection click is often heard; the proximity of the click to the S2 varies depending on the severity of stenosis. Splitting of the S2 results from prolonged ejection delay in the pulmonary valve component and may become fixed in severe pulmonary valve stenosis. The ECG typically demonstrates right axis deviation and features of right ventricular hypertrophy.
Mitral valve prolapse with mitral regurgitation may cause symptoms of palpitations. The murmur of mitral regurgitation is generally heard best at the apex. The central venous pressure is generally normal, and a right ventricular impulse would not be expected. Fixed splitting of the S2 is not heard in patients with mitral valve prolapse. The ECG is typically normal.
Key Point
- Fixed splitting of the S2 throughout the cardiac cycle and a right ventricular heave are characteristic clinical features of atrial septal defect.