MKSAP Quiz: New-onset cloudy vision
A 60-year-old man is evaluated for new-onset monocular cloudy vision of the left eye that began 4 hours ago. He has type 2 diabetes mellitus and coronary artery disease. His current medications are aspirin, simvastatin, lisinopril, metoprolol, and metformin.
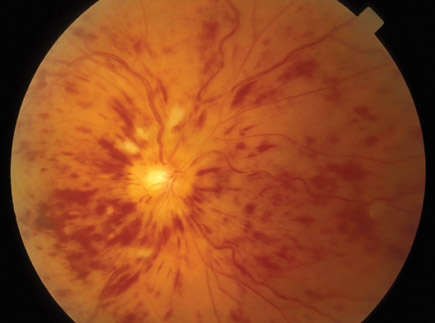
On physical examination, vital signs are normal. When a light is shined into his left eye it is not reactive, but shining a light in his right eye causes his left pupil to contract (left afferent pupillary defect). The visual acuity of the right eye is 20/30, that of the left eye is 20/120. Retinal findings are shown. The remainder of the examination is normal.
Which of the following is the most likely diagnosis?
A. Acute angle closure glaucoma
B. Central retinal artery occlusion
C. Central retinal vein occlusion
D. Retinal detachment
Answer and critique
The correct answer is C: Central retinal vein occlusion. This question can be found in MKSAP 16 in the General Internal Medicine section, item 61.
This patient most likely has central retinal vein occlusion (CRVO). Patients with CRVO experience acute onset of painless blurry vision due to reduced venous outflow and vascular edema in the eye. CRVO is characterized by optic disc swelling, dilated and tortuous veins, flame-shaped retinal hemorrhages, and cotton-wool spots (“blood and thunder”). Because the nerve supply to the eye remains intact but vision is decreased, an afferent pupillary defect in the affected eye may be present. CRVO is most commonly encountered in older patients with hypertension and atherosclerotic vascular disease. Cases have also been associated with acute carotid artery dissection and conditions associated with increased blood viscosity, such as polycythemia vera, sickle cell disease, and leukemia. Prognosis depends on the degree of visual impairment at the onset of symptoms. There is no generally accepted acute management, but a thorough investigation into possible etiologies should be undertaken.
Acute angle closure glaucoma is characterized by narrowing or closure of the anterior chamber angle, which impedes the trabecular drainage system in the anterior chamber, resulting in elevated intraocular pressure and damage to the optic nerve. Typical signs and symptoms include significant pain, diminished visual acuity, seeing halos around lights, a red eye, headache, and a dilated pupil. The globe may feel firm owing to increased intraocular pressure (often to 30 mm Hg or higher). Retinal examination may be normal or demonstrate optic cupping if chronic narrow-angle glaucoma is present.
Central retinal artery occlusion (CRAO) classically presents in a 50- to 70-year-old patient as a painless, abrupt blurring or loss of vision that occurs in the early morning hours—usually between midnight and 6 a.m. It results from an embolic or thrombotic event in the ophthalmic artery. It is typically unilateral. On examination, visual acuity is markedly diminished in the affected eye to either finger counting or light perception. There is an afferent pupillary defect. On funduscopic examination, the retina appears pale, either segmentally or completely. The fovea may appear as a cherry red spot. Interruption of the venous blood columns may be recognized with the appearance of “box-carring”—rows of slowly moving corpuscles separated by clear intervals. These findings are not present in this patient.
Symptoms of retinal detachment include diminished vision, photopsia (flashes of light), abrupt onset of multiple floaters in the vision, and metamorphopsia (wavy vision). Retinal detachment may result from trauma or occur spontaneously, particularly in persons with myopia. It is typically unilateral. On funduscopic examination, retinal detachment is characterized by distortion, folding, and tearing of the retina, which were not seen in this patient.
Key Point
- Central retinal vein occlusion is characterized by acute onset of painless blurry vision and optic disc swelling, dilated and tortuous veins, flame-shaped retinal hemorrhages, and cotton-wool spots (“blood and thunder”).


