MKSAP Quiz: Assessment of exertional dyspnea
A 70-year-old man with a history of a systolic murmur presents for further assessment of exertional dyspnea. He has had dyspnea his entire life, but has noted a recent deterioration in his exercise capacity. He has no other medical conditions and is on no medications.
On physical examination, his blood pressure is 120/70 mm Hg and pulse is 75/min and regular. The jugular venous pulse contour demonstrates a prominent a wave and the carotid pulses are normal. On cardiac examination, there is a parasternal impulse and a systolic thrill. The apical impulse is not displaced. An ejection click in close proximity to the S1 is heard along the left sternal border and second left intercostal space, which decreases in intensity with inspiration. A grade 4/6 early systolic murmur that increases with inspiration is best heard in the second left intercostal space without radiation to the carotid arteries. No diastolic murmur is noted.
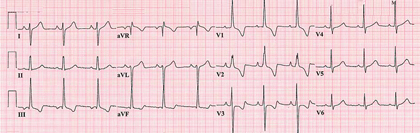
The electrocardiogram is shown. Chest radiograph demonstrates dilatation of the main pulmonary artery.
Which of the following is the most likely diagnosis in this patient?
A. Aortic valve stenosis
B. Atrial septal defect
C. Mitral valve regurgitation
D. Pulmonary valve stenosis
E. Tricuspid valve regurgitation
Answer and critique
The correct answer is D: Pulmonary valve stenosis. This question can be found in MKSAP 15 in the Cardiovascular Medicine section, item 6.
The patient has characteristic physical examination findings, electrocardiogram, and chest radiograph consistent with pulmonary valve stenosis. The jugular venous pulse contour demonstrates a prominent a wave. A right ventricular lift and systolic thrill are present. An ejection click is noted and is close to the S1, suggesting severe pulmonary valve stenosis. This sound decreases in intensity during inspiration (the only right-sided sound that decreases during inspiration). An early systolic murmur is noted over the pulmonary area. The electrocardiogram demonstrates right ventricular hypertrophy and right axis deviation. The chest radiograph demonstrates pulmonary artery dilatation. The diagnosis can be confirmed by echocardiography.
A bicuspid aortic valve is a more common cause of an ejection click than is congenital pulmonary valve disease, and it is associated with the development of aortic stenosis. The classic symptoms of aortic stenosis include dyspnea, angina, and exertional syncope. Aortic stenosis is characterized by small and late carotid pulsations, a late-peaking systolic murmur loudest in the second right intercostal space, absent splitting of S2, and a sustained apical impulse. The murmur characteristically radiates to one or both carotid arteries. Findings suggesting right ventricular hypertrophy would not be expected on physical examination or on the electrocardiogram.
The characteristic physical examination finding in atrial septal defect is fixed splitting of the a and v waves may be noted on jugular venous assessment. A right ventricular impulse is present. An ejection click may be audible if the pulmonary artery is enlarged but is less common than in patients with pulmonary stenosis. A pulmonary midsystolic murmur and a tricuspid diastolic flow rumble may be heard owing to increased flow through the valves from the left-to-right shunt. A systolic thrill, loud systolic murmur, and post-stenotic dilation of the pulmonary artery would not be expected in a patient with an isolated atrial septal defect.
Chronic mitral valve regurgitation is characterized by a holosystolic murmur at the apex that radiates to the axilla without respiratory variation. Mitral valve regurgitation may cause secondary pulmonary hypertension, but an ejection click and a loud early systolic murmur would not be expected with mitral valve regurgitation, even in the presence of pulmonary hypertension.
Tricuspid valve regurgitation causes a holosystolic murmur noted at the left sternal border. This characteristically increases with inspiration, but marked right ventricular hypertrophy and right axis deviation would not be expected on the electrocardiogram with this valvular lesion. The jugular venous pulse contour demonstrates a prominent v wave with tricuspid regurgitation, rather than a prominent a wave.
Key point
- Characteristic features of pulmonary valve stenosis include a prominent a wave in the jugular venous pulse contour, a parasternal impulse, an ejection click, a systolic thrill, and an early systolic murmur that increases with inspiration.


