MKSAP Quiz: new-onset atrial fibrillation
A 30-year-old woman is evaluated for management of new-onset atrial fibrillation. She has a history of tetralogy of Fallot that was repaired at age 18 months. She has had no cardiovascular concerns since then and has not had regular follow-up since childhood.
On exam, blood pressure is 120/70 mm Hg and heart rate is 70/min and irregular. The estimated central venous pressure is 10 cm Hv wave. The carotid examination is normal. The apical impulse is normal and there is a parasternal impulse. A grade 2/6 holosystolic murmur is noted along the lower left sternal border and increases with inspiration. A grade 2/6 early decrescendo diastolic murmur is also noted at the second left intercostal space; it also increases with inspiration.
An electrocardiogram demonstrates right bundle branch block and atrial fibrillation. The heart rate is 90/min.
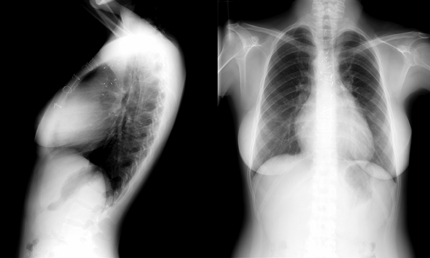
Chest radiographs are shown.
Which of the following is the most likely cause of this patient's atrial fibrillation?
A. Aortic and mitral valve regurgitation
B. Pulmonary and tricuspid valve regurgitation
C. Residual ventricular septal defect
D. Right ventricular outflow tract obstruction
Answer and critique
The correct answer is B. Pulmonary and tricuspid valve regurgitation. This question can be found in MKSAP 15 in the Cardiovascular Medicine section, item 116.
This patient has a history of tetralogy of Fallot with previous repair, which usually involves placement of a transannular pulmonary outflow tract patch. This causes severe pulmonary valve regurgitation, which is confirmed by the presence of a diastolic murmur that increases with inspiration, a parasternal impulse (right ventricular enlargement), and elevated central venous pressure. The holosystolic murmur at the left lower sternal border is characteristic of tricuspid regurgitation. Long-standing pulmonary valve regurgitation causes right ventricular enlargement and tricuspid annular dilatation with resultant regurgitation. The tricuspid regurgitation causes right atrial enlargement and increases the risk of atrial arrhythmias. The chest radiograph demonstrates features of right heart enlargement with a prominent right heart border (right atrium) and absence of the retrosternal air space (right ventricular enlargement). A right-sided aortic arch is also noted, which is present in 25% of patients with tetralogy of Fallot.
Tetralogy of Fallot is the most common form of cyanotic congenital heart disease, accounting for approximately 10% of all congenital defects. Although these defects have been successfully repaired for over 50 years, most patients with repaired tetralogy of Fallot have cardiac residua that may manifest with symptoms of dyspnea, heart failure, or arrhythmias years after repair. Life-long informed surveillance is recommended for patients with repaired tetralogy of Fallot. Patients with repaired tetralogy of Fallot are at increased risk of developing atrial arrhythmias due to atrial enlargement and prior atrial surgical incisions. These patients are also at risk of developing ventricular arrhythmias, which result primarily from dilatation and dysfunction of the right ventricle. Arrhythmias are a major cause of morbidity and mortality in patients with repaired tetralogy of Fallot.
Aortic valve regurgitation may occur in patients with repaired conotruncal abnormalities, such as tetralogy of Fallot. These patients may demonstrate progressive enlargement of the aorta and, eventually, aortic valve regurgitation may occur. The physical examination findings in this patient suggest pulmonary valve regurgitation rather than aortic valve regurgitation. The murmur of aortic regurgitation does not vary with respiration and is best heard in the second left intercostal space and down the left sternal border and would not cause right ventricular enlargement with a parasternal impulse. The pulse pressure is normal in this patient, and in a patient with aortic regurgitation, a wide pulse pressure would be expected.
A holosystolic murmur at the left sternal border that increases with inspiration is characteristic of tricuspid regurgitation rather than mitral valve regurgitation.
Residual or recurrent ventricular septal defect also occurs in patients with prior tetralogy of Fallot repair. A ventricular septal defect causes a loud systolic murmur that obliterates the S2 and is often associated with a palpable thrill. A displaced apical left ventricular impulse and mitral diastolic flow rumble would suggest a hemodynamically important ventricular septal defect causing volume overload.
Right ventricular outflow tract obstruction occurs commonly after repair of tetralogy of Fallot. However, the primary features include right ventricular hypertrophy rather than right heart enlargement. In addition, this patient's murmurs of tricuspid and pulmonary valve regurgitation would suggest that right ventricular outflow tract obstruction is not the cause of the patient's current clinical deterioration. The murmur of pulmonary stenosis is an early systolic murmur that increases with inspiration and is heard best at the second left intercostal space. It is associated with a loud P2 heart sound that is sometimes palpable.
Key point
- Pulmonary valve regurgitation is the most common residua after repair of tetralogy of Fallot.