MKSAP: Vision loss in one eye
A 68-year-old woman is evaluated in the emergency department for difficulty seeing out of her left eye. The symptoms were first present upon awakening 45 minutes earlier. She describes her vision as “looking through a dark veil.” Her right eye is unaffected. There is no associated pain, headache, muscle aching, or difficulty chewing, and no trauma or history of a similar episode. She has hypertension, hypercholesterolemia, and chronic open-angle glaucoma. Current medications are ramipril, hydrochlorothiazide, atorvastatin, aspirin, and timolol ophthalmic solution.
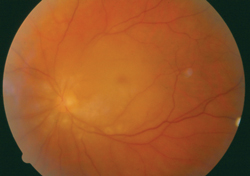
Vital signs are normal. Visual acuity in the right eye is 20/30, corrected for glasses; in the left eye, visual acuity is restricted to finger counting. Both globes are nontender to palpation. There is no conjunctival injection. Ophthalmoscopic examination of the right eye is normal. Findings in the left eye are shown.
Venous pulsations are noted. Pupils are equal. The right pupil reacts to direct and consensual light stimulus. The left pupil has sluggish response to direct light, but normal consensual response. Cardiac and neurologic examinations and electrocardiogram are normal.
Which of the following is the most likely diagnosis?
A. Acute angle-closure glaucoma
B. Acute occipital stroke
C. Central retinal artery occlusion
D. Central retinal vein occlusion
E. Retinal detachment
Answer and critique
The correct answer is C) Central retinal artery occlusion. This question can be found in MKSAP 15 in the General Internal Medicine section, item 51.
This patient presents with the acute onset of painless visual loss, which should immediately raise concern for an ischemic vascular event, in this case a central retinal artery occlusion (CRAO). CRAO classically presents in a 50- to 70-year-old patient, often in the early morning hours, with an abrupt but painless loss of vision. Risk factors include atherosclerosis, diabetes mellitus, hypertension, hypercholesterolemia, hypercoagulable states, and migraine. This patient has notable physical examination findings typical of CRAO: markedly diminished visual acuity; an afferent pupillary defect; and a pale fundus, with a “cherry red spot” near the fovea. Central visual acuity may be preserved if the retina is perfused by the cilioretinal artery.
CRAO represents a “stroke to the eye.” Interventions to restore perfusion are essential, as permanent visual loss may result within 90 to 100 minutes from symptom onset, although the most effective intervention is not known. Immediate consultation with an ophthalmologist is essential. Ocular massage for 15 minutes, agents to lower the intraocular pressure, and lying the patient flat may help the plaque or clot to migrate and can be initiated immediately.
Acute angle-closure glaucoma can result in acute visual loss that is typically painful, in contrast to this patient's presentation. Additionally, patients present with headache, seeing halos around lights, conjunctival injection, a pupil that is mid-dilated and sluggish or fixed in reaction to light, and sometimes a clouded cornea.
An acute stroke may cause loss of vision. Neurologic findings in this patient are absent, other than for monocular visual loss, which would be unusual as the sole presenting feature of an occipital stroke. Furthermore, the funduscopic findings are typical of CRAO and would not be seen in an ischemic event to the occipital lobes.
Central retinal vein occlusion (CRVO) may also present with the abrupt onset of painless, monocular visual loss. In contrast to CRAO, however, the retina is notable for hemorrhages, “cotton wool” spots, or the classic “blood and thunder” appearance of extensive edema and hemorrhages.
Symptoms of retinal detachment include the relatively sudden and painless onset of floaters. The peripheral vision is usually affected first, and then symptoms may progress over days or weeks to involve the central vision. The abrupt onset of near complete monocular visual loss and the appearance of the retina in this patient make retinal detachment unlikely.
Key point
- The acute onset of painless visual loss suggests the possibility of a central retinal artery occlusion, which is a medical emergency.